New Paper Alert, with not 1 but THREE of my advisees!
Download the paper HERE
Study Context The MMPI-3 is the latest revision in the line of the MMPI family of instruments, and includes updated norms and scale revisions. Included within the revisions on the MMPI-3 are changes to several of the well-validated MMPI-2-RF over-reporting scales. Three scales include new or reworked items, in addition to the renorming process. In this study (just accepted for publication in The Clinical Neuropsychologist) we examine how effective they were in a simulation, symptom coached design.
We picked a four condition design PTSD, mTBI, comorbid PTSD+mTBI since validity scales on the MMPI are designed to detect different symptom sets of invalid responding (e.g., infrequent psychopathology on F and Fp or infrequent somatic/neurological concerns on Fs, FBS, or RBS). PTSD offers a largely internalizing pathology symptom-set while TBI is largely somatic/cognitively focused. Few studies have evaluated comorbid conditions in validity scale feigning, and symptom sets have previously moderated scale effectiveness (both in simulation designs and in meta-analytic reviews). Given the high frequency of PTSD and mTBI overlap in military/veteran samples, this provided a great context for us to examine the MMPI-3’s scale utility. We coached participants on symptoms via a brief verbal description they and a written symptom description derived from Wikipedia on each condition.

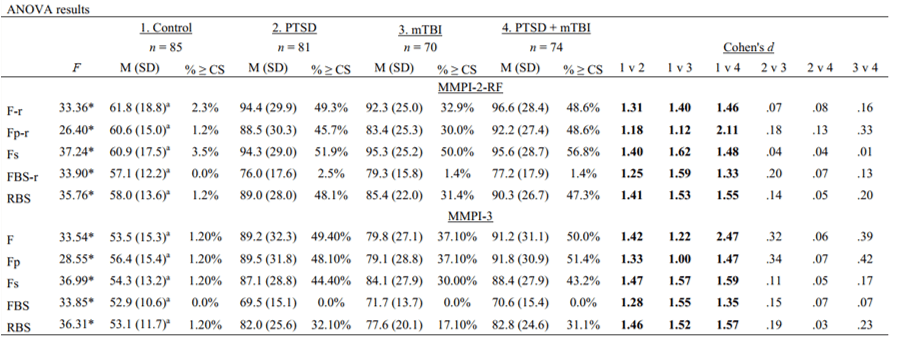
Results Across the four conditions, the scales had effect sizes similar to those in other studies on symptom validity test effectiveness (e.g., other over-reporting scales on measures like the MMPI-2, MMPI-2-RF, or PAI) compared to control (d ~ 1.0 to 1.5) but negligible effects between diagnostic conditions. Our effects are different than the other simulation study out there (Whitman et al., 2021); however, ours are closer to what would expect. In our original paper we listed both the MMPI-2-RF and the MMPI-3, as well as incremental analyses but our final report is only the MMPI-3. I’ve provided both analyses below. Results are similar across instruments, which isn’t surprising given the correlation between the scales. In general, using the MMPI-3 over-reporting scales at their recommended cut scores means that you can be confident about those invalidating as being most likely exaggerating or misrepresenting symptoms but you may miss many others who are misrepresenting their symptoms.
We also calculated sensitivity and specificity across a variety of scale cut scores and, in general, scale performance was consistent with past work on broadband validity scales (high specificity, low sensitivity, and mean scores below recommended cut values).
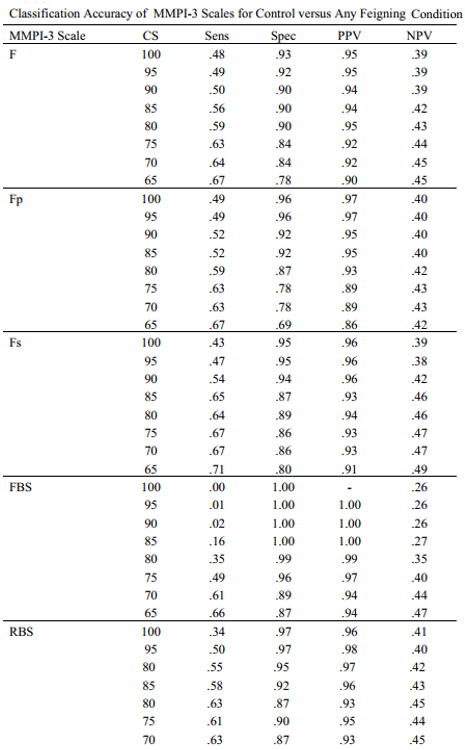
The lack of effect between diagnoses of dissimilar symptom sets (e.g., somatic/cognitive versus psychopathology) was unexpected given past study on moderation. Likewise, FBS was distinct in its performance relative to the other scales – people elevated less on it and rarely invalidated it. This is curious since its designed for head injury litigants. Our FBS findings may reflect the simulation study design; however, since it is the only scale with that pattern of results, further research on a reason why this may have occurred is also warranted. Replication with military and veteran samples given the high relevance to referral concerns is also needed.
